|
There is one "best" thing in the world to help reduce anxiety, to increase mental clarity and ability to focus, and for increased general well-being: Deep Breathing!
You can live for days without food, up to a month, approximately 44,640 minutes. You can live for days with water, up to a week, approximately 10,080 minutes or more. But you can only live for 3 to 5 MINUTES -- without OXYGEN! Deep breathing is IMPORTANT... Yet, most of us are unable to spend more than a few minutes bringing our awareness to our breath. And this is usually only during a "sigh" or the point in the day when the stress of the day was too great that we take what we think is a healthy deep breath. The problem is usually with the mechanics or "way" we take that deep breath. Granted any extra oxygen that enters the system is going to be somewhat beneficial and potentially reduce anxiety or center you, that is as long as you are not hyperventilating. How to deep breathe: The most important aspect of deep breathing is making sure when taking an "in-breath" that your stomach is extended outward. Your diaphragm, the main muscle for breathing will be contracted. When you breath out, the diaphragm will be relaxed, and your stomach will move in. It is most important to focus your awareness on this in/out movement of your breath and your diaphragm. If you notice, the "in" breath happens when your stomach is moving out, and when your stomach moves in you should be exhaling the breath "out." So one way to picture this is with a +/- vs -/+. There are never two "+'s," i.e. NEVER an in-breath/in-stomach, nor two "-'s," i.e. NEVER an out-breath/out-stomach. It is ALWAYS one or the other but NEVER both "ins" or both "outs"... In stomach - Out Breath, +/- Out stomach - In Breath, -/+ Or, Out Stomach - In Breath, -/+ In Stomach - Out Breath, +/- but NEVER +/+ or -/- This may seem difficult to control in the beginning but after time and some perseverance you will be able to re-establish a healthy breathing pattern that will last throughout the day and there is a lot more to learm but this is the "best" place to start. You should try to learn to deep breath the same way you attempt to learn a new language or to play a musical instrument: Multiple (3-5 times) short (2-5 minutes) per day. By Mathew Quaschnick
0 Comments
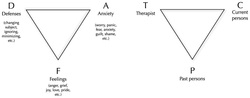 Intensive Short-term Dynamic Psychotherapy (ISDP) utilizes two maps, Triangle of Conflict and of Person, for assisting the therapeutic processing of client behavior.
ISDP favors this schematic for directing the behavioral as well as interventional material within the immediate moment and moments of the session as they are produced in the here and now. The triangle of conflict represents the dynamic flow of the client's unconscious material. The triangle of person is meant to pictorially represent the basic reality that the therapist-client relationship. There are three main components each representing an active conscious or unconscious dynamic in any given relationship. The client draws from these relationships: e.g. the therapist "T," past persons "P," and current persons "C" to determine how they should interact with someone. The client may respond utilizing the "triangle of conflict" when the therapist attempts to interact with the client while utilizing behavioral patterns that the client has utilized in the past. For example: If the therapist requests information about the client's presenting concern, let's say, "general depression," and the client talks about how they have not been able to "get to work on time" then this could be a defensive, or "D" response. The D response is meant to block the feelings, or "F" response, associated with the actual depressive feelings. If the client was able to answer the question about their depressive feelings then there may have been a chance for processing the emotions. However, the D response by the client instead wards off anxiety, and is an "A" response, in the triangle. All of the points: D, A and F--are connected and each time that the therapist asks a question or implements an intervention there is a chance for one of the resulting points [D, A and F] to be utilized by the client. It is not as simple as always wanting to get an F response but more so of the therapist being actively aware of each response and then associating the triangle of conflict responses back to the Triangle of People so that the client and therapist can begin to understand the historical as well as current relationships that have and continue to contribute to the client's main presenting problem, aka general depression--but it could be any mental health concern. By Mathew Quaschnick Looking at Psychology Today's "Compassion Matters: Eight Ways to Actively Fight Depression"10/17/2013 The article "Eight Ways to Actively Fight Depression" describes eight unique ways to take control some of the most common symptoms of depression. I will, over-time, be incrementally summarizing the ways Lisa Firestone, Ph.D. describes her methods for fighting depression.
1. "Recognize and Conquer Your Critical Self Attacks" This is one symptom that people suffering from depression most often complain. The critical attack can take the from of "a critical, self-destructive mentality that interferes with and distracts us from our daily lives." This is normally associated with a low self esteem and manifests as a "critical inner voice." This can be internalized at a very early age and makes it one of the most difficult symptoms to actively engage toward positive change outside of a therapeutic relationship. This is not to say that working outside of a therapeutic relationship is in vain but the intimate connection between self-esteem and your sense of self is difficult to separate from your self, alone and by one's self. Dr. Firestone asks you to view the negative self talk as "parasites" that keep you in your bed during a regular physical sickness. But unlike the physical parasites, which you have no control over, Dr. Firestone advises that you have control over the negative self talk by bringing your awareness to them and actively identifying them as "alien point[s] of view." She then asks you to critically analyze the thoughts via a projection of them onto those whom you love: "would you think such cruel thoughts about a friend or family member?" Ultimately Dr. Firestone wishes that you should have compassion upon yourself and that "awareness" of your destructive thoughts will lead to more clear and realistic interpretation of yourself. By Mathew Quaschnick 2. "Think About What You Could Be Angry At" The masked feelings of anger can be contributing to your depressive feelings. There is little doubt that unexpressed anger toward an individual, situation or emotionally significant object needs an outlet. Dr. Firestone briefly describes how this is the potential case regarding depression. She makes the suggestion to begin talking to others. This is a wonderful start but not everyone is comfortable talking about feelings of anger and not everyone has someone to healthfully begin this conversation. However, there are positive and therapeutic options people can begin utilizing to assist in the healthy expression of anger: (1) The long term solution may be to begin talk therapy, and that is not a shameless endorsement of my work. I have help countless individuals with anger management and depression is a normal response to anger as Dr. Firestone states. (2) Exercise! Beginning a daily or 3x per week workout routine, incorporating a martial arts practice, utilizing a heavy bag for boxing, etc... (3) Deep breathing: The most important aspect of deep breathing is making sure when taking an in-breath that your stomach is extended outward. Your diaphragm, the main muscle for breathing will be contracted. When you breath out, the diaphragm will be relaxed, and your stomach will move in. (4) Emergency stop gap intervention: If there is no time to perform the above options the next best effort is simply removing yourself, at the time of the feelings, from the source of anger. You can then "live to fight another day" and not inappropriately express your anger. http://www.psychologytoday.com/blog/compassion-matters/201110/eight-ways-actively-fight-depression By Mathew Quaschnick
|
UPTOWN THERAPY MPLSEdited and composed by Mathew Quaschnick
Sort articles by clicking below on ARCHIVES or CATEGORIES.
MENTAL HEALTH THERAPY
LOCATION AND HOURS:
1406 West Lake St. #204 Minneapolis, MN 55408
Monday - Friday: 9-5 PM with limited evening appointments
Archives
March 2017
Categories
All

|
 RSS Feed
RSS Feed
|
Uptown Therapy is wonderful. I have benefited greatly these past 8 months and am sure to continue. |