|
"What gives?" Therapy can be a very difficult process to begin, to continue and then even more to complete. While therapy is a complex process there are specific parts of it that, if recognized, can make the whole process much more fluid and potentially productive. So instead of trying to tackle a massive question like, "how does therapy work?," instead, let's discuss one aspect: "What moves?"
Everyone engaged in therapy wants therapy to move forward and at some point come to a positive and healthy conclusion. Regardless of an unexpressed desire that happens to short-circuit or obstruct the forward movement, and this does happen much more often than one would think, the fact that someone actively attends sessions implies that they do want to get past their current problems. So, if we focus on the "what moves" therapy, then we may be able to keep ourselves somewhat more focused and productive in therapy? I would not be so bold as to state that there is only one component in therapy that moves therapy, but I would like to put forward that there can be one thing that does contribute greatly to this forward progression: Desire. It, like therapy, is a very complicate idea. It has been discussed throughout entire books and by many authors: Jacques Lacan, Jean Baudrillard, Gilles Deleuze. One way of looking at desire could be to put in contrast to wishing for something. "I wish that I didn't have this problem." or "I want ("want" being the more common usage for word "desire") to be free of this problem." A person having a wish is the same as someone desiring something but for someone to desire something they are also taking an active role in attaining whatever it is desired. This doesn't mean that they will get it and while wishing is a very important part of the psyche, desire has this active component. So desire is active and potentially "what moves" in therapy because, simply put, moving things are active. Wishes are important, "wish fulfillment," but unless there is the active or desiring component the wish remains stagnant and inactive--similar to wishing upon a star--AND good too, if that is getting your childhood creativity moving -- wink, wink! However in therapy we want to focus on things that can be actively worked on. The "what moves" therapy forward toward lasting change, and a positive therapeutic outcome. Wishing is not desiring but you can desire to attain a wish. Is there another way can we think to get desire moving? Otherwise we are just saying desire (is) active and wishing (is) inactive? Everyone gets thirsty, everyone needs to eat and more so everyone NEEDS to breathe. These behaviors are "hard-wired" instincts and all people are compelled to satisfy them. My article on deep breathing has a fun way of describing this. Most complex organisms have instincts but there is only one that desires. Jacques Lacan's theories about psychoanalysis has the most thorough and extended explanation of desire and its relationship to therapy. He states that while all animals, those with complex nervous systems, have instincts; but, only those that have language have desire. An ability to communicate does not mean or qualify one to have language. Language = Desire. Language is distinguished by Lacan via the "Symbolic Register" or the ability to manipulate symbols. Lacan distinguishes purely animal communication from human language by the human's ability to make symbolic representations, i.e. written language symbols, e.g. hieroglyphs, pictographic/ideographic. The animal does not manipulate such symbols, while they do definitely have the ability to manipulate sounds and even concepts through their body movements, e.g. a pack of wolves hunting, they do not have a system of externally representable symbols, i.e. a language, such that distinguishes homo sapiens. The reason that this is important for the movement of therapy and positive therapeutic outcomes is that our language overwrites our instincts and thereby creates desire. This does not happen in animals. Animals have "pure" instincts and do not seek or desire "Lucky Charms" cereal instead of "Cheerios" to satisfy the instinct of hunger. Again, the choice or preference for one or the other is complicated but the animal does not have a network of symbolic associations related to their food. The animal could prefer Lucky Charms but they wouldn't because of the cartoon character or because they are "magically delicious." "What moves?" Well desires! But desires can be thwarted or actively stopped by others whose own desire is in conflict with yours. This can cause problems. Especially when you are a young, vulnerable child who is desiring very basic needs: Security, both emotional and physical. If these needs are not met then psychological complications can ensue. It can be the place of therapy to get things moving and my article on the movements and stoppages in therapy can be a place to learn more about this. By Mathew Quaschnick
1 Comment
 “How does therapy move forward?” and “why doesn't it seem to sometimes?” Nearly everyone who begins therapy will come up against both of these questions. Both questions are potentially very complicated to answer. Therefore, it will be the place of this article to only touch upon a basic way of illustrating some of the more general components of the processes involved. Then some of the complications people may confront will be introduced. As long as we keep it basic I believe that you will be able overlay or insert your personal experiences and then maybe recognize and prevent the stoppages and encourage the forward progressions.
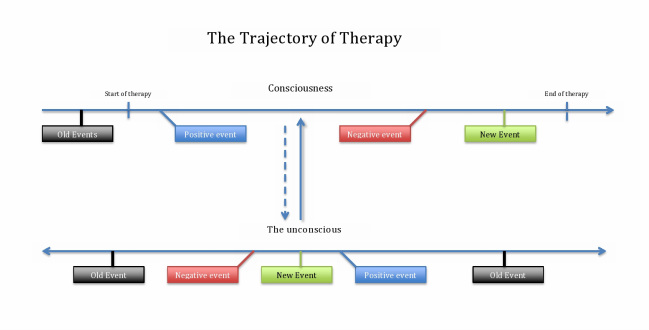
The accompanying graph has two horizontal lines, which are labeled “Consciousness” and “The unconscious.” These can be thought of as the individual’s ability to be aware, i.e. conscious, and the reality that sometimes we are not so aware of some things, i.e. the unconscious. An example of how we are not aware or are unconscious of something is simply your name. Your name remains unconscious until someone calls you by it or you see it written or as you are possibly thinking about it just now. So, back to the graph: The top line labeled “Consciousness” can be thought of as the materially physical and the temporal, time-dependent aspect. It is the part that you experience in you daily life and the part that your immediate awareness recognizes. The past, present and future are all on this line and you recall it based on its chronological order. The “Start of Therapy” could easily be the “start of the day” or the “start of the workday,” it represents the first session of therapy. Therapy continues down this line with positive, negative or “new” events. Therapy, however, does not move forward as easily and obviously as would your workday or any other day of your life. Therapy is, or at least should be, a very different experience from your normal daily life. The main reason why therapy is vastly different is the therapist should be looking for what comes out of your unconscious. This is unlike the interactions you will have with other people in your daily life. Normally people are just concerned with the “face-value” of what you are saying and how it effects them: “You want a Kit-Kat,” “Well I like Snickers.” The therapist is listening for your likes and dislikes, for sure, but they are not then comparing them to their own. The therapist is paying attention to your unconscious desire to talk about candy bars instead of the original reason you started therapy. Now back to “why does therapy seem to stop?” Positive and negative events occur all throughout therapy. One day therapy seems to click and you really feel like “I get this and I like it,” but then the next week there seems to be something off and for that matter you don’t even recall any of the positive events from the last week. A very simple way of illustrating this is the dynamic between the two lines on the graph. It is very easy to be happy or fulfilled by therapy on a good day where you experience what seems to be a positive movement forward; however, when that event is over, and for that matter even when a negative event is over, the idea of the event moves from your consciousness to the unconscious. Now the trick is that once it is in the unconscious there is no particular temporal placement for it and it is not easily recalled. The positive or negative events are both moved into the unconscious and are held there with all of the other events that have occurred in your lifetime waiting for a reason to be recalled consciously or being recalled unconsciously or unexpectedly because there was an associated event, similar to when your name is called out to you. The unconscious does not “discriminate” what goes in or what comes out and does not therefore “stop” therapy. What will stop therapy is the lack of communication between the therapist and yourself. The unconscious is always communicating to your consciousness. It is not always communicating in the language that you recognize. Why were you taking about candy bars again? It is the place of the therapist, their skill and experience, to build the relationship and rapport between them self and yourself, that is the communication between you and the therapist is model for the communication between you and your unconscious. This constant communication between yourself and the therapist mimics your unconscious and consciousness communication and will keep the therapy moving forward. By Mathew Quaschnick Transference is a psychoanalytic term originating in the early work of Sigmund Freud. The term has been utilized to refer to the same "experience" in therapy but, depending upon the theorist discussing the concept, it is always described in many different ways. This makes the term very unique, very powerful but also very difficult and sometimes useless.
The experience of transference occurs on the side of the the person engaged in therapy, that is it originates in the client's psyche. It is a psychological process that moves from the psyche of the client, via projection, onto the therapist. "Countertransference" is the term utilized when the therapist has the experience themselves. Just as the client is normally unconscious of the projection, so will the therapist not normally recognize or be conscious of the projection he imposes onto the client. The therapist may have the skill to prevent themselves from projecting and awareness to notice that they are projecting depending upon their level of skill and self-awareness. The fact that there is a projection is what distinguishes transference, regardless of whether it originates in the therapist or client. However, to maintain a sense of simplicity and to entertain the idea in a basic way transference always begins in the client and moves toward, or is projected at the therapist. The essential qualifying factor for transference is that an emotion is engaged by and then elicited, projected by the client at the therapist and that the client then believes, consciously or unconsciously (more on the importance of it not needing to be conscious below), that the therapist behaved or acted in a way to warrant the emotion. The therapist, if conscious that he is eliciting the emotion can then investigate/analyze "why" the emotion was elicited, but if he is unconscious that it was elicited due to "transference" then the therapist is, at best without a direction to assist the client in healthfully processing the emotion--which is not good; and at worst, the therapist may become offended or lash out at the client--which is detrimental. The therapist should know that the he should -- NOT -- engage on a personal, or directly emotional level with the client otherwise the therapist risks the relationship and any potential positive therapeutic value that is inherent to the projected emotion. Jaques Lacan utilized what he called the "L schema" to assist would be therapists (Psychoanalysis calls a therapist a "psychotherapist" and a client and "analysand"). Without going into too great of detail the basic idea behind Lacan's schema is that the therapist should not engage with the client from a person-to-person, or ego based perspective. They should instead engage the client from the Symbolic Register (or Symbolic Level). They should attempt to remain in a virtual state of reflection and not submit to the emotions. What is the symbolic value of the emotion and NOT "why the hell did you [the client] call me a bastard!?!" If the therapist doesn't know to NOT respond on the level of ego, or the Imaginary Register, then the therapy will more then likely devolve into an argument; thereby, greatly negatively impacting the relationship and potentially blocking any further positive therapeutic outcome. Transference can come from either direction but how the trained representative reacts to the individual situation is the key to any positive therapeutic outcome. By Mathew Quaschnick |
UPTOWN THERAPY MPLSEdited and composed by Mathew Quaschnick
Sort articles by clicking below on ARCHIVES or CATEGORIES.
MENTAL HEALTH THERAPY
LOCATION AND HOURS:
1406 West Lake St. #204 Minneapolis, MN 55408
Monday - Friday: 9-5 PM with limited evening appointments
Archives
March 2017
Categories
All

|
 RSS Feed
RSS Feed
|
Uptown Therapy is wonderful. I have benefited greatly these past 8 months and am sure to continue. |